Oxalate and its acid form oxalic acid are organic acids that are primarily from three sources: the diet, from fungus such as Aspergillus, Penicillium, and possibly Candida, and also from human metabolism.
Foods especially high in oxalates include spinach, beets, chocolate, peanuts, wheat bran, tea, cashews, pecans, almonds, berries, and many others. A complete list of high oxalate foods can be found here.
High oxalate in the urine and plasma was first found in people who were susceptible to kidney stones. Many kidney stones are composed of calcium oxalate. Stones can range in size from the diameter of a grain of rice to the width of a golf ball. It is estimated that 10% of males may have kidney stones some time in their life.
Such crystals may also form in the bones, joints, blood vessels, lungs, and even the brain. In addition, oxalate crystals in the bone may crowd out the bone marrow cells, leading to anemia and immunosuppression.
Oxalates in the urine have also been shown to be much higher in individuals with autism. In one study, 36% of children on the autistic spectrum had values higher than 90 mmol/mol creatinine, the value consistent with a diagnosis of genetic hyperoxalurias, while none of the non-autistic children had values this high.
As shown in the table below, both mean and median values for urine oxalates are substantially higher in autism compared to the general population. As a matter of fact the mean oxalate value of 90.1 mmol/mol creatinine is equal to the lower cutoff value for the genetic hyperoxalurias. The median value in autism is six times the normal median value and the mean value in autism is five times the normal mean value.
| Statistic | Normal urine oxalate | Autistic Spectrum urine oxalate |
| Mean | 15.7 | 90.1 |
| Median | 11.5 | 90.1 |
| Std dev | 10.8 | 75.8 |
Researcher Susan Owens discovered that the use of a diet low in oxalates markedly reduced symptoms in children with autism and PDD. For example, a mother with a son with autism reported that he became more focused and calm, that he played better, that he walked better, and had a reduction in leg and feet pain after being on a low oxalate diet. Prior to the low oxalate diet, her child could hardly walk up the stairs. After the diet, he walked up the stairs very easily. Many hundreds of children with autism throughout the world are now being placed on this diet with good results.
Further Potential Dangers of High Oxalates
Oxalate crystals may cause damage to various tissues. The sharp crystals may cause damage due to their physical structure and may also increase inflammation. Iron oxalate crystals may also cause significant oxidative damage and diminish iron stores needed for red blood cell formation. Oxalates may also function as chelating agents and may chelate many toxic metals such as mercury and lead. Unlike other chelating agents, oxalates trap heavy metals in the tissues.
In addition to autism and kidney disease, individuals with fibromyalgia and women with vulvar pain (vulvodynia) may suffer from the effects of excess oxalates.
The most convenient way of testing oxalates is with the Organic Acids Test (OAT) from The Great Plains Laboratory, Inc.
The Organic Acids Test checks for the presence of:
- Oxalic acid (oxalates) – Tests for all forms of oxalic acid and its salts or conjugate bases, oxalates
- Arabinose – Important Candida indicator which strongly correlates with oxalates
- Glycolic acid (glycolate) – Indicator of genetic disease of oxalate metabolism called Hyperoxaluria type I due to a deficiency in the enzyme activity of alanine glyoxylate amino transferase (AGT).
- Glyceric acid (glycerate) – Indicator of genetic disease of oxalate metabolism called Hyperoxaluria type II due to a deficiencyin an enzyme (GRHPR) that has two biochemical activities: glyoxylate reductase (GR) and hydroxypyruvic reductase (HPR).
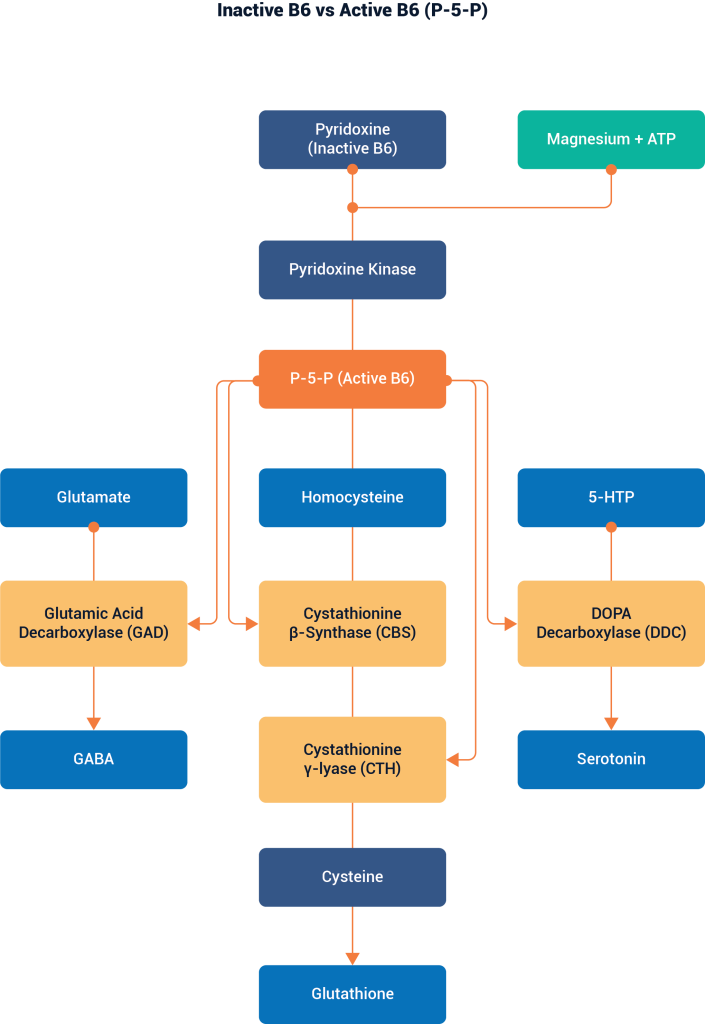
- Pyridoxic acid – Indicator of vitamin B-6 intake. The enzyme activity alanine glyoxylate amino transferase (AGT) requires vitamin B-6 to eliminate glyoxylic acid or glyoxylate, a major source of excess oxalates.
- Furandicarboxylic acid, hydroxy-methylfuroic acid – Markers for fungi such as Aspergillus infection, one of the proven sources of oxalates
- Bacteria markers – A high amount of bacterial markers may indicate low values of beneficial bacteria such as Lactobacilli species that have the ability to destroy oxalates.
- Use antifungal drugs to reduce yeast and fungi that may be causing high oxalate. Children with autism frequently require years of antifungal treatment. I have noticed that arabinose, a marker used for years for yeast/fungal overgrowth on the Organic Acids Test (OAT) at The Great Plains Laboratory, is correlated with high amounts of oxalates, and arabinose has been found to be an important fuel for fungal oxalate production. Candida organisms have been found surrounding oxalate stones in the kidney.
- Give supplements of calcium citrate to reduce oxalate absorption from the intestine. Citrate is the preferred calcium form to reduce oxalate because citrate also inhibits oxalate absorption from the intestinal tract. The best way to administer calcium citrate would be to give it with each meal.
- Try N-Acetyl glucosamine to stimulate the production of the intercellular cement hyaluronic acid to reduce pain caused by oxalates.
- Give chondroitin sulfate to prevent the formation of calcium oxalate crystals.
- Vitamin B6 is a cofactor for one of the enzymes that degrade oxalate in the body and has been shown to reduce oxalate production.
- Increase water intake to help to eliminate oxalates.
- Reduce excessive fats in the diet, which may cause elevated oxalate if the fatty acids are poorly absorbed because of bile salt deficiency. Non-absorbed free fatty acids bind calcium to form insoluble soaps, reducing calcium’s ability to bind oxalate and reduce oxalate absorption. If taurine is low in the Amino Acids Test, supplementation with taurine may help stimulate bile salt production (taurocholic acid), leading to better fatty acid absorption and diminished oxalate absorption.
- Probiotics may be very helpful in degrading oxalates in the intestine. Individuals with low amounts of oxalate-degrading bacteria are much more susceptible to kidney stones. Both Lactobacillus acidophilus and Bifidobacterium lactis have enzymes that degrade oxalates.
- Increase intake of essential omega-3 fatty acids, commonly found in fish oil and cod liver oil, which reduces oxalate problems.
- Reduce intake of omega-6 fatty acids. High amounts of the omega-6 fatty acid, arachidonic acid, are associated with increased oxalate problems. Meat from grain fed animals is high in arachidonic acid.
- Take supplements of vitamin E, selenium, and arginine which have been shown to reduce oxalate damage.
- Undertake a low oxalate diet. This may be especially important if the individual has had Candida for long periods of time and there is high tissue oxalate buildup. There may be an initial bad reaction lasting several days to a week after starting the diet since oxalates deposited in the bones may begin to be eliminated as oxalates in the diet are reduced.
References
- Tsao, G. Appl Microbiol. 1963 May; 11(3): 249-254. Production of Oxalic Acid by a Wood-Rotting Fungus.
- Takeuchi H Konishi T, Tomoyoshi T. Observation on fungi within urinary stones. Hinyokika Kiyo. 1987 May;33(5):658-61.
- Lee SH, Barnes WG, Schaetzel WP. Pulmonary aspergillosis and the importance of oxalate crystal recognition in cytology specimens. Arch Pathol Lab Med. 1986 Dec;110(12):1176-9.
- Muntz FH. Oxalate-producing pulmonary aspergillosis in an alpaca. Vet Pathol. 1999 Nov;36(6):631-2.
- Loewus FA, Saito K, Suto RK, Maring E. Conversion of D-arabinose to D-erythroascorbic acid and oxalic acid in Sclerotinia sclerotiorum. Biochem Biophys Res Commun. 1995 Jul 6;212(1):196-203.
- Fomina M, Hillier S, Charnock JM, Melville K, Alexander IJ, Gadd GM. Role of oxalic acid overexcretion in transformations of toxic metal minerals by Beauveria caledonica. Appl Environ Microbiol. 2005 Jan;71(1):371-81.
- Ruijter, G.J.G., van de Vondervoort, P.J.I. & Visser, J. (1999) Oxalic acid production by Aspergillus niger: an oxalate-non-producing mutant produces citric acid at pH 5 and in the presence of manganese. Microbiology 145, 2569–2576.
- Ghio AJ, Peterseim DS, Roggli VL, Piantadosi CA. Pulmonary oxalate deposition associated with Aspergillus niger infection. An oxidant hypothesis of toxicity. Am Rev Respir Dis. 1992 Jun;145(6):1499-502.
- Takeuchi H, Konishi T, Tomoyoshi T. Detection by light microscopy of Candida in thin sections of bladder stone. Urology. 1989 Dec;34(6):385-7.
- Ghio AJ, Roggli VL, Kennedy TP, Piantadosi CA. Calcium oxalate and iron accumulation in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2000 Jun;17(2):140-50.
- Ott SM, Andress DL, Sherrard DJ. Bone oxalate in a long-term hemodialysis patient who ingested high doses of vitamin C. Am J Kidney Dis. 1986 Dec;8(6):450-4.
- Hall BM, Walsh JC, Horvath JS, Lytton DG. Peripheral neuropathy complicating primary hyperoxaluria. J Neurol Sci. 1976 Oct;29(2-4):343-9.
- Sahin G, Acikalin MF, Yalcin AU. Erythropoietin resistance as a result of oxalosis in bone marrow. Clin Nephrol. 2005 May;63(5):402-4.
- Sarma AV, Foxman B, Bayirli B, Haefner H, Sobel JD. Epidemiology of vulvar vestibulitis syndrome: an exploratory case-control study. Sex Transm Infect. 1999 Oct;75(5):320-6.
- http://www.thevpfoundation.org/effective_treatment.htm
- Shirane Y, Kurokawa Y, Miyashita S, Komatsu H, Kagawa S. Study of inhibition mechanisms of glycosaminoglycans on calcium oxalate monohydrate crystals by atomic force microscopy. Urol Res. 1999 Dec;27(6):426-31.
- Chetyrkin SV, Kim D, Belmont JM, Scheinman JI, Hudson BG, Voziyan PA. Pyridoxamine lowers kidney crystals in experimental hyperoxaluria: a potential therapy for primary hyperoxaluria.
- Sangaletti O, Petrillo M, Bianchi Porro G. Urinary oxalate recovery after oral oxalic load: an alternative method to the quantitative determination of stool fat for the diagnosis of lipid malabsorption. J Int Med Res. 1989 Nov-Dec;17(6):526-31.
- Kumar R, Mukherjee M, Bhandari M, Kumar A, Sidhu H, Mittal RD. Role of Oxalobacter formigenes in calcium oxalate stone disease: a study from North India. Eur Urol. 2002 Mar;41(3):318-22.
- Azcarate-Peril MA, Bruno-Barcena JM, Hassan HM, Klaenhammer TR. Transcriptional and functional analysis of oxalyl-coenzyme A (CoA) decarboxylase and formyl-CoA transferase genes from Lactobacillus acidophilus. Appl Environ Microbiol. 2006 Mar;72(3):1891-9.
- Baggio B, Gambaro G, Zambon S, Marchini F, Bassi A, Bordin L, Clari G, Manzato E. Anomalous phospholipid n-6 polyunsaturated fatty acid composition in idiopathic calcium nephrolithiasis. J Am Soc Nephrol. 1996 Apr;7(4):613-20.
- Gambaro G, Bordoni A, Hrelia S, Bordin L, Biagi P, Semplicini A, Clari G, Manzato E, Baggio B. Dietary manipulation of delta-6-desaturase modifies phospholipid arachidonic acid levels and the urinary excretion of calcium and oxalate in the rat: insight in calcium lithogenesis. J Lab Clin Med. 2000 Jan;135(1):89-95.
- Santhosh Kumar M, Selvam R. Supplementation of vitamin E and selenium prevents hyperoxaluria in experimental urolithic rats. J Nutr Biochem. 2003 Jun;14(6):306-13.
- Pragasam V, Kalaiselvi P, Sumitra K, Srinivasan S, Varalakshmi P. Pragasam V, Kalaiselvi P, Sumitra K, Srinivasan S, Varalakshmi P. Counteraction of oxalate induced nitrosative stress by supplementation of l-arginine, a potent antilithic agent. Clin Chim Acta. 2005 Apr;354(1-2):159-66. Epub 2005 Jan 19.
- Takenouchi KAso K, Kawase K, Ichikawa H, Shiomi T. On the metabolites of ascorbic acid, especially oxalic acid, eliminated in urine, following administration of large amounts of ascorbic acid. J Vitaminol (Kyoto). 1966 Mar 10;12(1):49-58.
- Curhan, G. C., Willett, W. C., Speizer, F. E., Stampfer, M. J. Intake of vitamins B6 and C and the risk of kidney stones in women. J Am Soc Nephrol 10:4:840-845, Apr 1999
- Dolske MC, Spollen J, McKay S, Lancashire E, Tolbert L. A preliminary trial of ascorbic acid as supplemental therapy for autism. Prog. Neuropsycho-pharmacol Biol Psychiatry. 1993 Sep;17(5):765-74.

Warren Maginn is a Clinical Nutritionist, College Lecturer and Public Educator specialising in the optimisation of health through the principles of Functional Medicine and a highly individualised approach to personal care. As an active National Association member and Chief Scientific Advisor to RN Labs, Warren is passionate about assisting practitioners and students to gain greater technical insights from current functional medicine understanding and how to apply this knowledge in clinical practice.